
Blood-based cancer monitoring is changing quickly, and several different tests are now available or in development to help doctors look for tiny traces of cancer in the blood after or during treatment. These tests are often called circulating tumor DNA (ctDNA) or “liquid biopsy” tests, and they are being studied as tools to:
- Check for molecular residual disease (MRD) after surgery or other curative‑intent treatment
- Estimate the risk that cancer may come back
- Monitor how well treatment is working over time
Because this field is evolving, no single test is right for every situation. Different ctDNA and liquid biopsy approaches have different strengths and limitations, and most are still being refined through research.
What ctDNA and liquid biopsy tests do
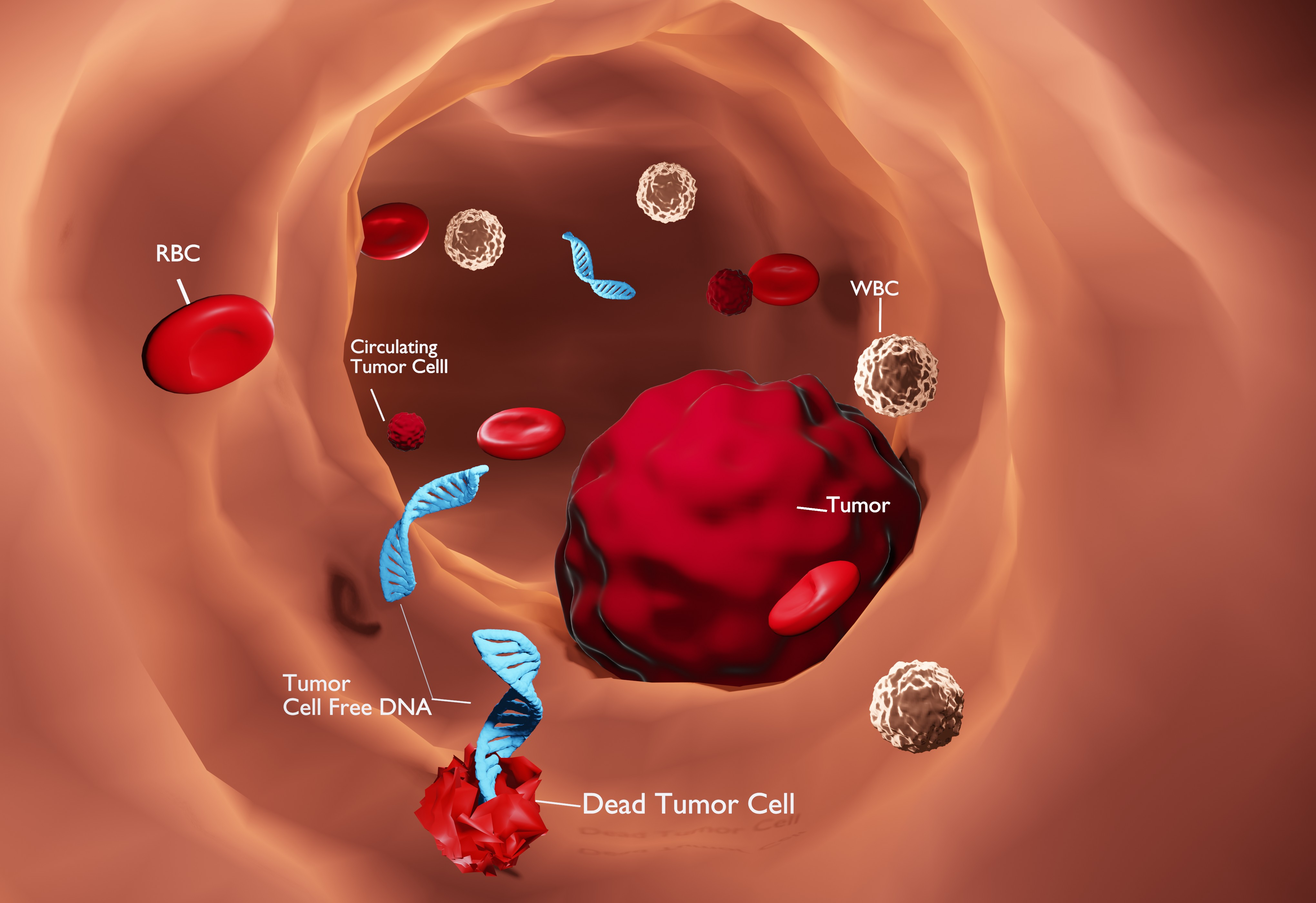
ctDNA tests look for small fragments of tumor DNA that have broken off cancer cells and entered the bloodstream. Some tests are tumor‑informed, meaning the lab first studies the patient’s tumor tissue to identify specific mutations, then builds a personalized blood test that tracks those mutations over time. Other tests are tumor‑naïve (blood‑only) and analyze a standard panel of genes in blood samples without needing tumor tissue.
In addition to ctDNA, some newer approaches also look at circulating tumor cells (CTCs)—whole cancer cells that have entered the bloodstream—to gather information about tumor burden and changing markers such as PD‑L1.
Signatera and other ctDNA options
One well‑known tumor‑informed ctDNA test is Signatera, which creates a personalized assay based on the unique DNA changes in each patient’s tumor. Signatera has been studied in several cancer types, including colorectal and breast cancer, and research has shown that:
- A positive result after surgery or treatment is often linked to a higher chance that the cancer may come back.
- A negative result can be reassuring, although it does not guarantee that recurrence will never happen.
Signatera has received FDA Breakthrough Device designations in certain settings, reflecting its potential clinical value, but like other ctDNA tests, it is still being incorporated into guidelines and practice step by step.
There are also other commercial and academic ctDNA assays—both tumor‑informed and blood‑only—that are being used or studied in various cancers. Some may offer faster turnaround times or require no tumor tissue, but in some studies they have shown less separation between high‑ and low‑risk groups compared with tumor‑informed tests, especially in early‑stage disease. Because head‑to‑head comparisons are limited, most experts recommend choosing a test based on the specific cancer type, stage, available evidence, and test access, rather than assuming one brand is always best.
New research using circulating tumor cells (CTCs)
Beyond ctDNA, researchers are also exploring ways to use circulating tumor cells to monitor cancer. In May 2026, CelLBxHealth announced a partnership with AdventHealth to use its Parsortix CTC platform in two large observational studies, ACTION and SUNRISE.
- These studies will enroll people with colorectal, gastrointestinal, and lung cancers and will track how CTC counts and other markers change over time with chemotherapy and supportive care.
- The research also pairs blood‑based monitoring with remotely delivered exercise programs, to see whether lifestyle interventions can improve treatment tolerance and possibly influence tumor biology.
CTC‑based testing is not as widely used in routine care as ctDNA today, but these trials may help clarify how CTC information could complement ctDNA and imaging in the future.
What this means for patients
For patients, the growing number of ctDNA and liquid biopsy options is both promising and confusing. Key points to keep in mind:
- No test is perfect. A positive ctDNA result does not always mean the cancer will definitely come back, and a negative result does not guarantee that it will not.
- Different cancers, different evidence. The amount of data supporting ctDNA testing varies by cancer type and stage. In some settings, results may already influence treatment decisions; in others, they are mainly used within clinical trials.
- Choice of test matters. Tumor‑informed and blood‑only tests work differently, and your oncologist may recommend one based on your specific cancer, prior treatments, and whether tumor tissue is available.
- CTC testing is emerging. CTC‑based monitoring, like the CelLBxHealth/AdventHealth studies, is still largely research‑focused but may eventually offer another layer of information alongside ctDNA.
If you are considering ctDNA or other liquid biopsy testing, ask your care team:
- What tests are available for my type and stage of cancer?
- How would a positive or negative result change my treatment plan, if at all?
- Is this test part of routine care, a clinical trial, or both?
- What are the costs and insurance coverage considerations?
Understanding these options—and their limits—can help you and your oncology team decide whether ctDNA or CTC monitoring fits into your overall treatment and follow‑up plan.



